| Blog Summary |
|---|
| The Neonatal Intensive Care Unit (NICU) has significantly improved the outcomes of preterm newborns, low birth weight newborns, and newborns with medical conditions. Hospitals classify newborns' care into four levels, from a normal nursery to a full NICU, based on how much support a newborn needs at birth. This blog breaks down what each level actually involves, who works there, and how doctors decide which one a newborn needs. |
Not every newborn who's born needs the same kind of medical support. Some go straight to a well-newborn nursery with their mother. Others need to stay back for a few extra days just to be watched more closely, and a smaller group needs round-the-clock intensive care from hospital staff right from birth. Hospitals plan for newborn care by organising what's called the levels of neonatology care, each one built for a different degree of medical need. This blog gets into what each level actually means and what changes along the way, plus how doctors decide where a newborn belongs.
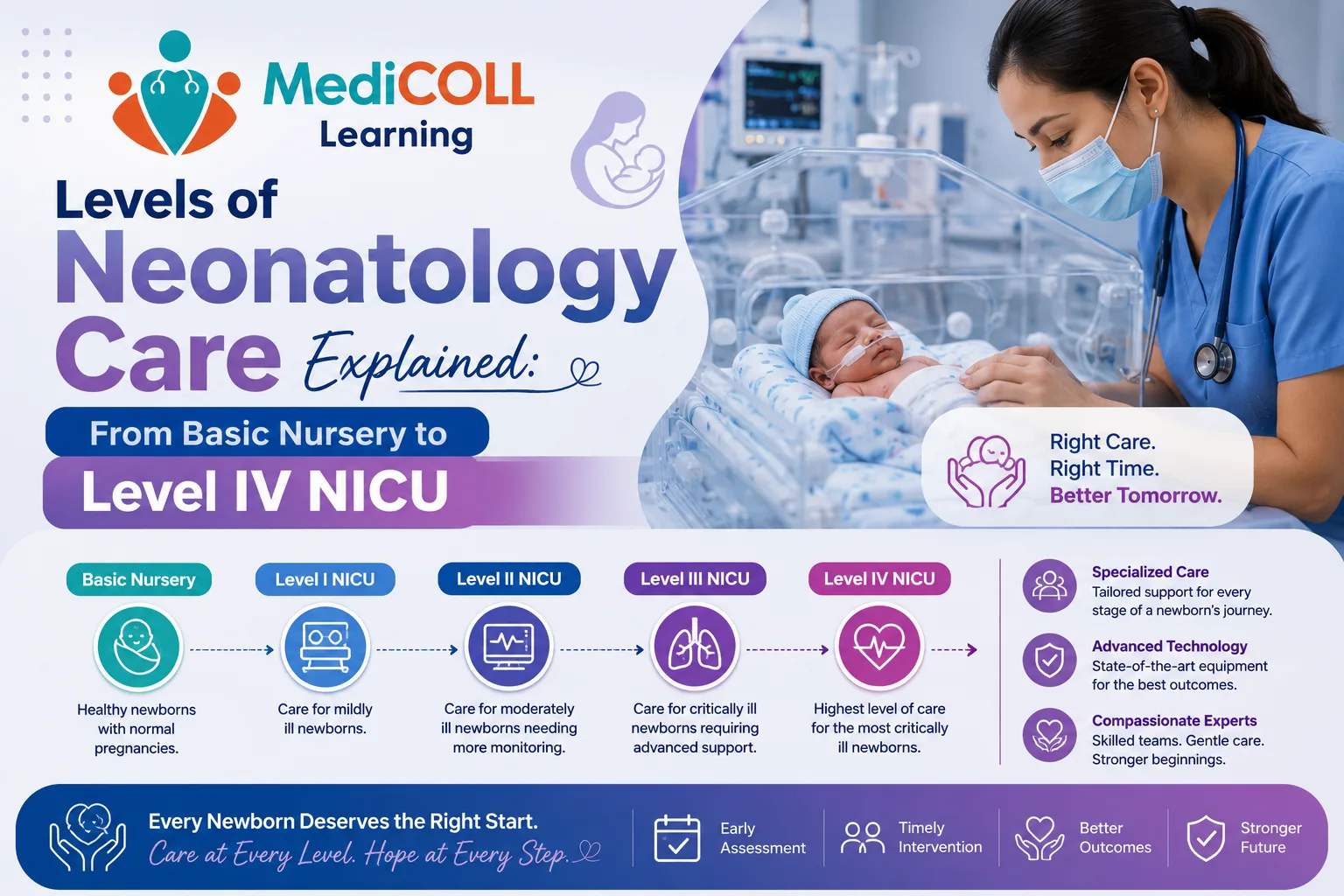
Neonatal care levels are split into four stages. Level I through Level IV based on how sick or premature a newborn is and how much equipment and staff that care requires. A newborn born healthy and full-term might never see anything past Level l
NICU is a specialised hospital ward that provides advanced medical and nursing care for newborns. These include newborns with low birth weight, those with severe health complications like infections, breathing disorders, or congenital conditions, and premature newborns born before 37 weeks. NICU, in the strict sense, only refers to Level III and IV. Level I and II cover everything before that.
Neonatology care in hospitals is classified by level to match a newborn's specific medical needs with the appropriate technology, resources, and clinical expertise. Placing a newborn who needs ventilator support in a unit that doesn't have one, or doesn't have staff trained to run one can be unsafe for the newborn.
This kind of standardisation also makes better use of hospital resources. High-risk deliveries get directed to facilities that already have the right equipment in place, which tends to mean faster recovery too. Smaller hospitals usually stop at Level I or II. Bigger hospitals, often regional, carry Level III and IV, since those need specialists, equipment, and round-the-clock staffing that not every hospital can provide.

Level I is the well-newborn nursery. This is where a healthy, full-term newborn at ≥ 37 weeks goes right after delivery. The newborn usually rooms in with the mother rather than staying in a separate ward. There's no underlying medical condition to manage.
Staff keep an eye on basic parameters like temperature, feeding, and weight, and they're trained to step in fast if something looks off. A Level I nursery typically has resuscitation equipment on hand in case of emergency but the day-to-day work is closer to routine newborn care.
Level II is called the special care nursery. This level is for moderately premature newborns, typically born after 32 weeks, and for newborns over 1,500 grams who still need closer monitoring than a standard nursery provides.
Most of these newborns are expected to improve within days. This level of neonatal care offers short-term breathing support like Continuous Positive Airway Pressure (CPAP). It also provides feeding tube assistance and IV medications for the newborns.
A Level II nursery has a handful of incubators and phototherapy units, and nurses usually look after two or three newborns at a time. If a newborn's condition worsens unexpectedly, the unit is set up to stabilise them quickly before transferring to a higher level of care.
Level III handles newborns who are critically unwell, as well as those born very premature or weighing less than 1,500 grams. Ventilators, continuous monitoring, and IV nutrition are standard care for those newborns.
Nurses stay close to just one or two newborns during a shift, since conditions can change within minutes. A Level III NICU can also manage most surgeries a newborn might need, though the most complex cases, such as heart surgery requiring bypass, are usually transferred to a specialised facility.
Level IV is the top of the system, reserved for the most complex and critically ill newborns, including those with severe congenital birth defects. A Level IV NICU offers the highest level of care, including pediatric surgical repair and advanced imaging. It also involves specialised treatments like extracorporeal membrane oxygenation (ECMO).
What changes between Level III and IV is who's available on-site which are paediatric surgeons, cardiologists who can perform complex heart repairs, and specialists across nearly every paediatric subspecialty.
| Level | Who It's For | What Stands Out |
|---|---|---|
| Level I | Healthy, full-term newborns | Rooming-in, routine newborn care |
| Level II | Moderately premature newborns or short-term monitoring needs | Incubators, phototherapy, 1 nurse per 2-3 newborns |
| Level III | Seriously ill or very premature newborns | Ventilators, continuous monitoring, 1 nurse per 1-2 newborns |
| Level IV | Newborns needing complex surgery or subspecialist care | On-site paediatric surgeons, regional referral hub |
Decisions around neonatal care services usually start before birth. If a pregnancy is high-risk, say the mother has diabetes, or labour starts very early, doctors often plan the delivery at a hospital that already has a higher-level unit available.
The medical team quickly evaluates the newborn in the first few minutes after birth to determine the appropriate tier of care. These criteria include gestational age, birth weight, respiratory stability and surgical necessity.
Newborns before 32 weeks of gestation usually need more advanced tiers of care. The same goes for those with a birth weight under 1,500 grams (about 3.3 pounds), who get routed past the basic tiers. A need for mechanical ventilation or continuous positive airway pressure (CPAP) automatically escalates the care tier as well, and congenital conditions that require immediate surgery place a newborn in the highest tier straight away.
These markers help the team to decide whether a newborn can stay with the mother or needs to move straight to a higher level of care. However, close monitoring by the neonatal healthcare team is required as a newborn's condition can change at any time.
The full form of NICU is Neonatal Intensive Care Unit. It is a specialised ward for the newborns who are severely ill, or have serious complications like breathing issues or congenital disorders. Premature newborns born before 37 weeks and newborns with low birth weight are also placed in NICU.
PICU (Pediatric Intensive Care Unit) is an intensive care unit for infants and children up to 18 years of age, while NICU is specifically for newborns. Newborns in the NICU may need to transfer to a PICU if their care needs extend beyond the newborn period. For example, if they need ongoing breathing tube support, a tracheostomy, feeding tubes, or other long-term medical care. The transfer depends on the hospital and the newborn's condition.
Levels of Neonatology Care are categorised into four stages. They range from basic well-baby nurseries to the highly specialised Level IV NICU. Each level comes with its own guidelines for staffing, equipment and the kind of interventions available.
Q. Can Parents Stay With Their Newborn in the NICU?
Yes, parents can generally stay with their newborn in the NICU. Most units allow 24-hour access these days, rather than fixed visiting hours. Skin-to-skin contact is usually encouraged once the baby is stable enough. Skin- to-skin contact has a measurable effect as it helps to regulate a baby's heart rate and breathing. Newborns who get this kind of regular contact tend to recover sooner and have short hospital stay. Apart from that, every hospital has its own rules around hand hygiene, gowning, and how many visitors are allowed at the bedside.
© Copyrights Medicoll All rights reserved.